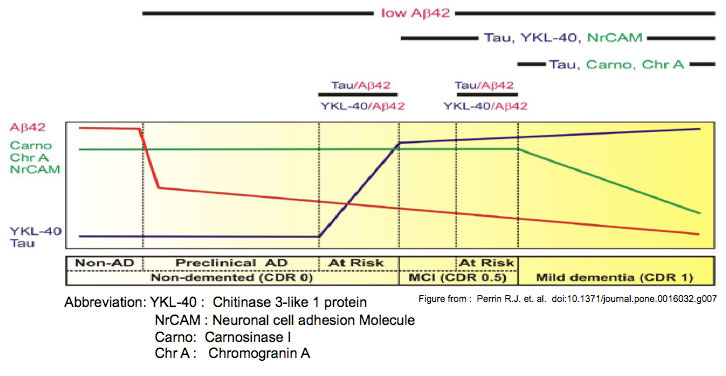
The horizontal bar (below) describes the early
clinicopathological progression from cognitive normalcy without AD
pathology (‘Non-AD’) to mild dementia in six stages. As depicted by the
curves above, Non-AD CSF has high Ab42 (red line), high chromogranin A
(Chr A), carnosinase I (Carno I) and NrCAM (green line), and low YKL-40
and tau (blue line). Reduced CSF Ab42 correlates with amyloid plaque
deposits, the first sign of neuropathologically identifiable AD
(‘preclinical AD’). CSF Ab42 appears to decrease further as cognition
declines from normal (Clinical Dementia Rating [CDR] 0) to very mild
cognitive impairment (MCI, CDR 0.5) to mild dementia (CDR 1). When
considered as ratios with Ab42, CSF markers of neuroinflammation (e.g.
YKL-40) and neurofibrillary tangle pathology (e.g. tau) appear to
increase before and predict the onset of very mild cognitive impairment
(MCI, CDR 0.5), defining a CDR 0 group ‘At Risk’ for cognitive decline
[9,15,137]; YKL-40 and tau also appear to be higher among those who
progress rapidly from very mild to mild dementia, defining a CDR 0.5
group ‘At Risk’ for impending cognitive decline [137,230]. Reductions in
synapseassociated (NrCAM, chromogranin A) and neuronal (carnosinase I)
proteins, and increases in YKL-40 and tau mirror the progression and
anatomical spread of synaptic and neuronal losses, gliosis and tau
pathology associated with cognitive decline, and can be used to define
CDR 0.5 and CDR 1.
Perrin R.J. et al. Doi:10.1371/journal.pone.0016032.g007